This is a case of a late middle-aged man with a big obstructing gallstone. His medical history is remarkable for morbid obesity with metabolic syndrome including ASCVD with previous MI and stroke, HTN, and DM II. He was also a multi-decade smoker with severe emphysema, and recently elevated liver enzymes. He had an obstructive stone in the common bile duct, and an ERCP was done to remove it. During the procedure, the stone was noted to be 4 cm in diameter. The stone was broken up and the treating physician had to use a basket to get the fragments out. The decedent seemed to tolerate the procedure well, but was found unresponsive at home three days later.
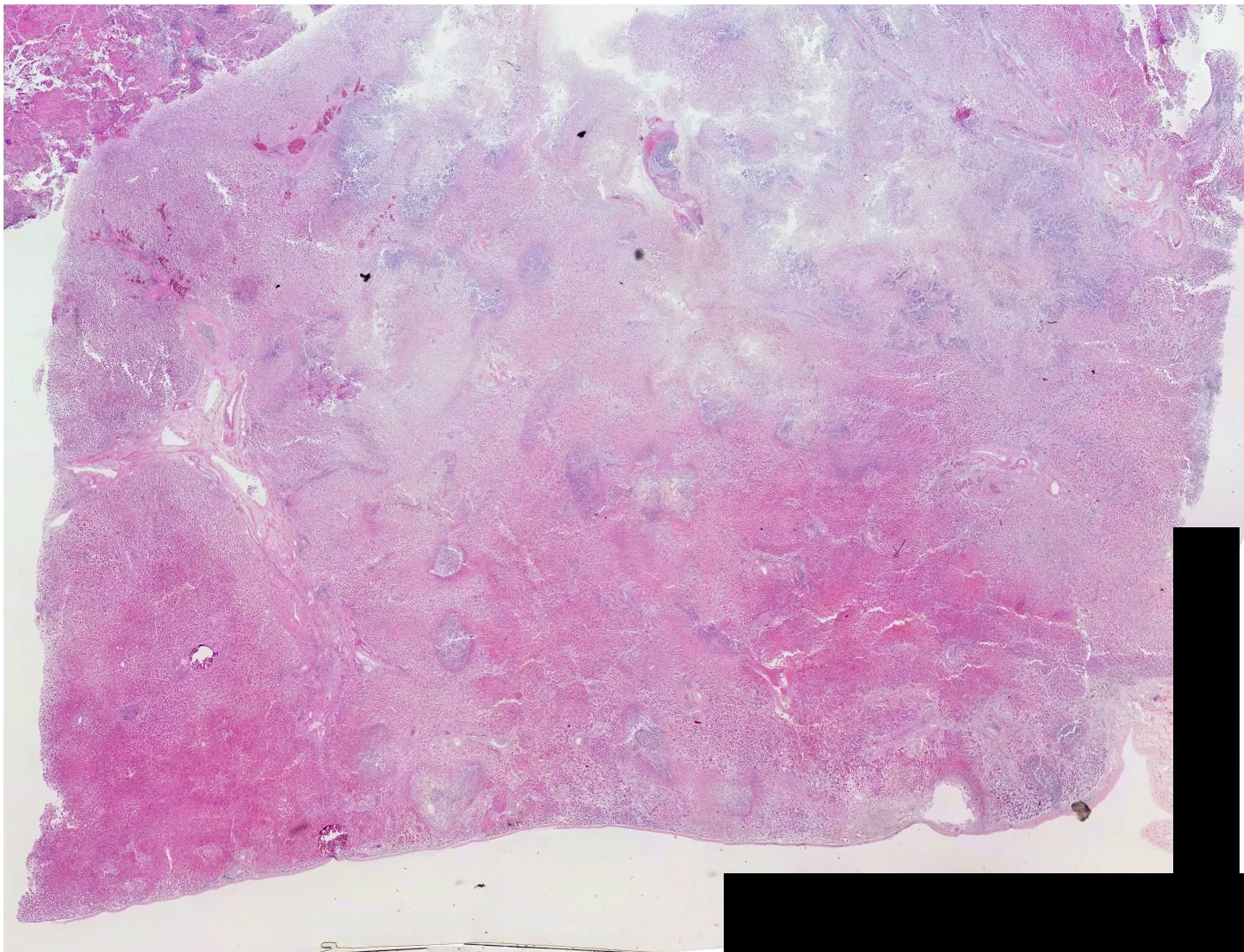
Autopsy confirmed the decedent’s antemortem chronic diagnoses. Examination of the gallbladder revealed it to be dilated but not obviously inflamed, and it contained 10 small (0.2-0.6 cm) faceted dark stones. Examination of the liver revealed a couple of foci of green cavitation and necrosis:


On histologic evaluation, this was a bunch of necrotic tissue:
Within this are little mini-abscesses that are a bit blue (arrows):
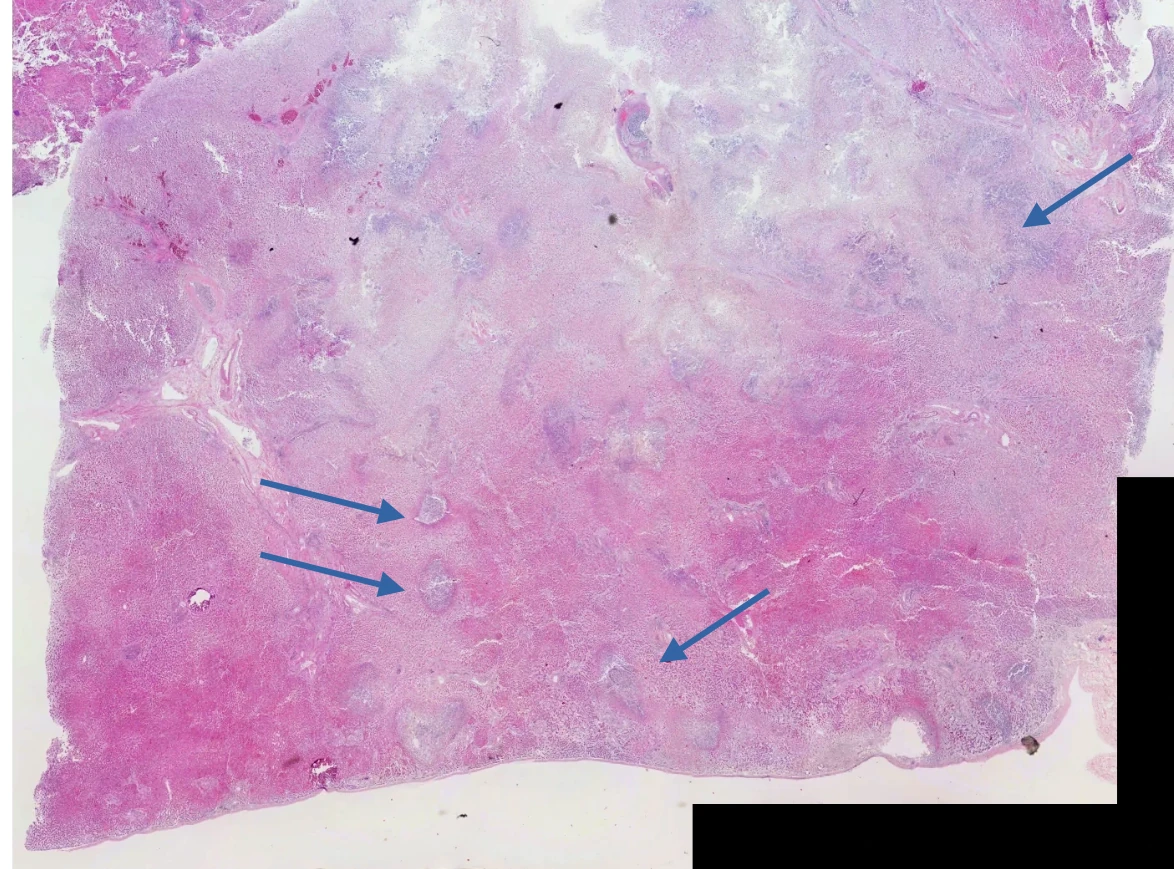
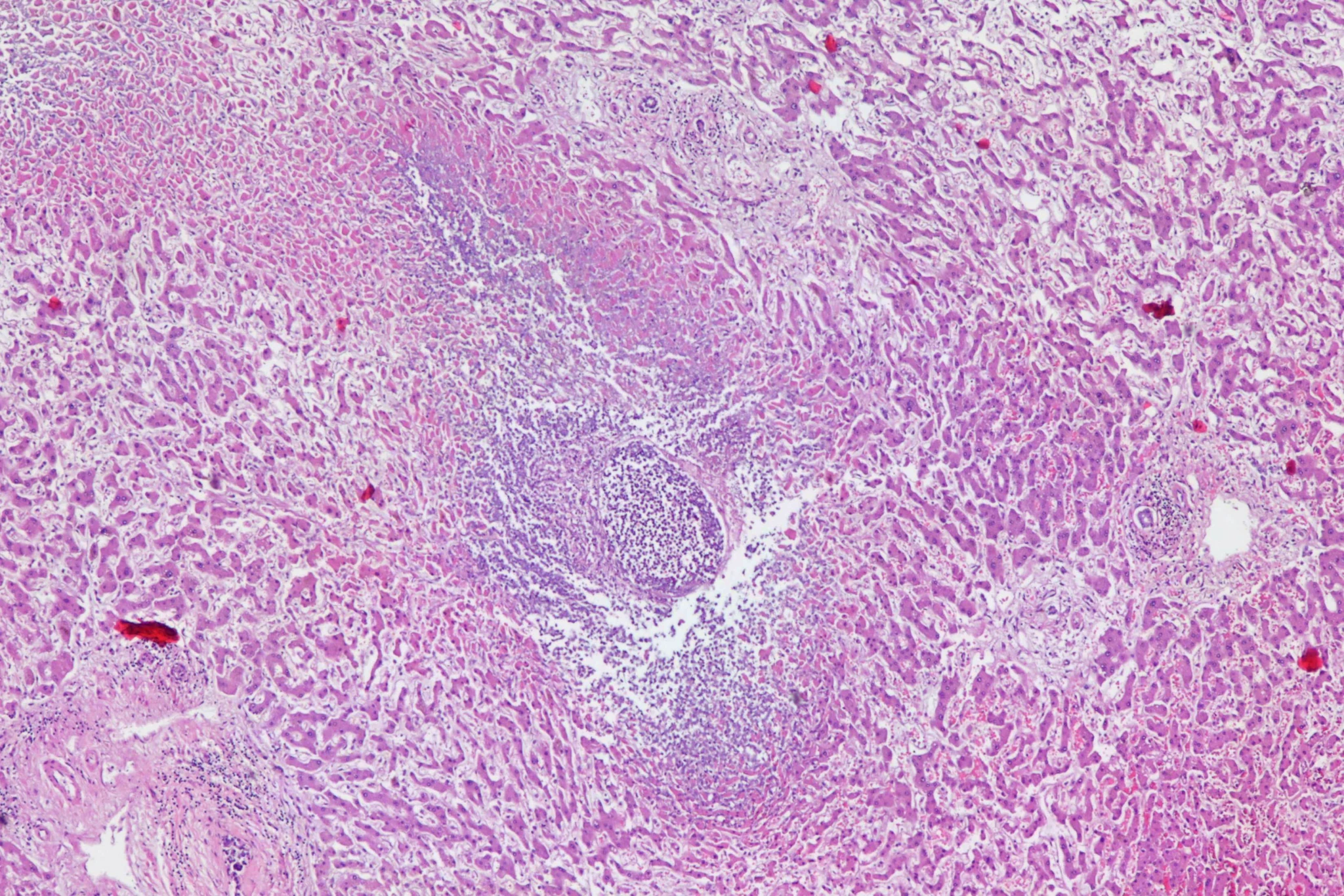
Here’s some medium magnification of some of these areas:

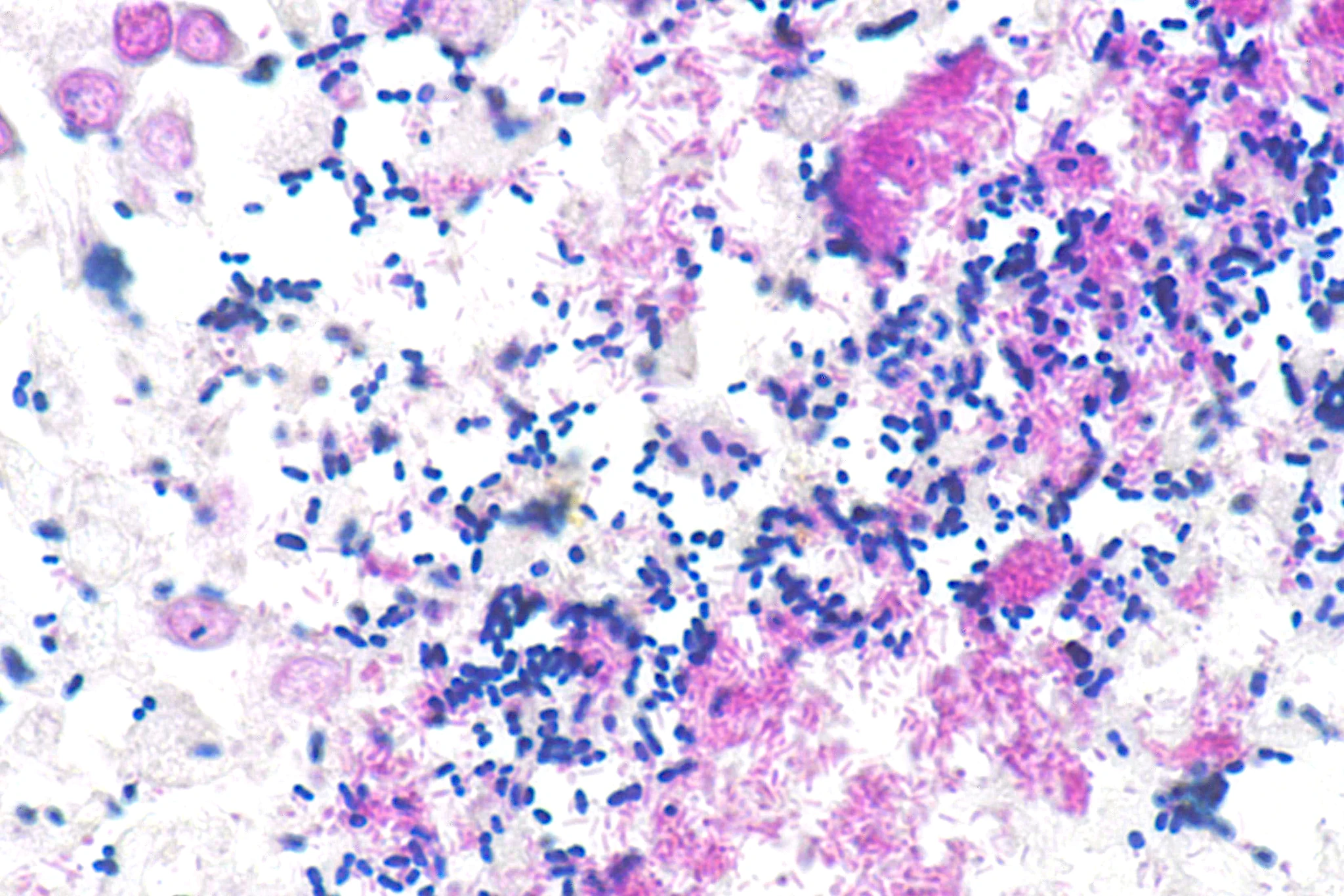
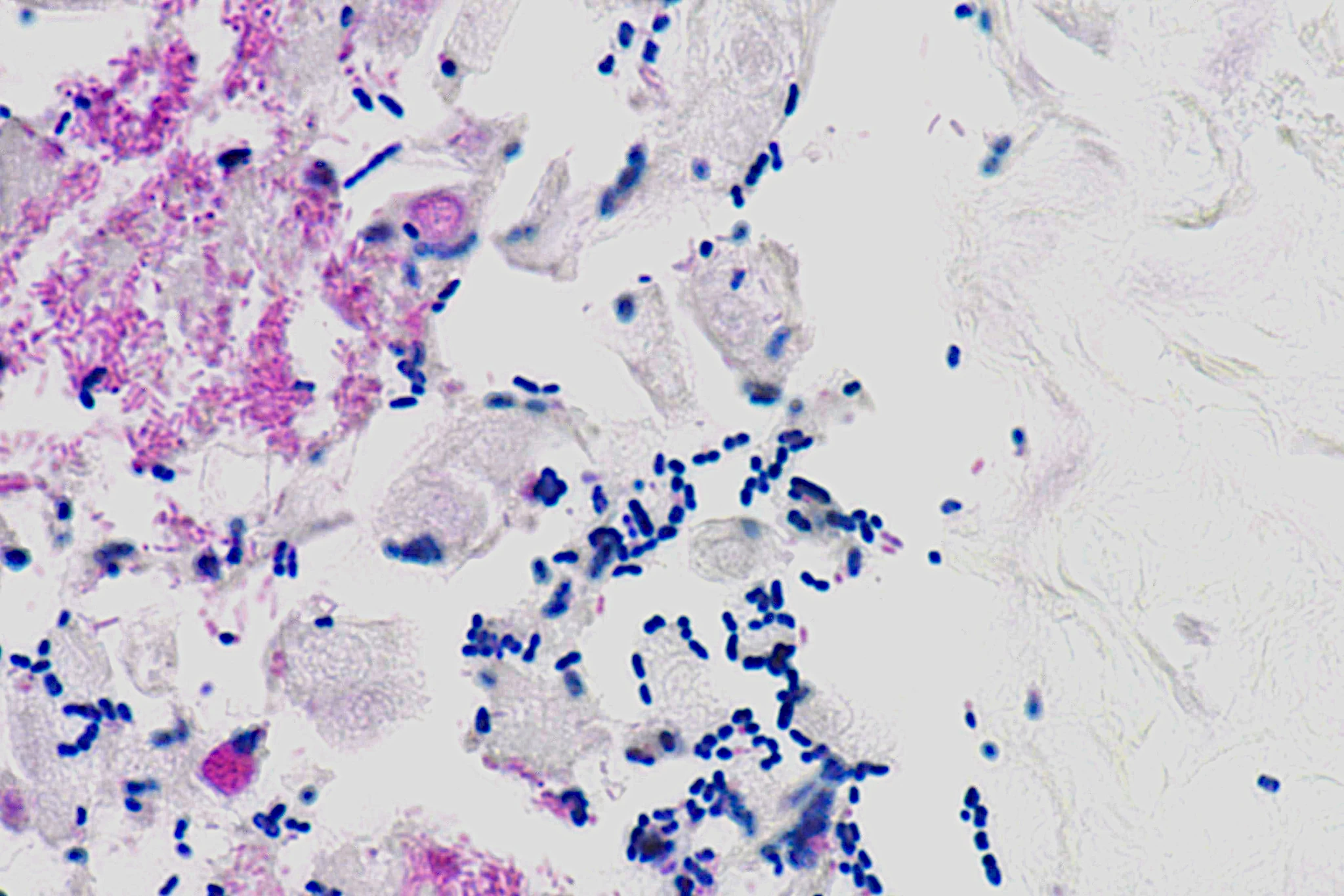
With Gram stain, there are lots of little blue dots:

Which, under oil, are clearly diplococci:
It turns out that there’s an increased risk of bacteremia/sepsis/cholangitis/etc from ERCP due to the need for irrigation, which can push bugs up into the biliary system. In one prospective study, almost 30% of patients had “sustained” bacteremia following the procedure(1). In another study of 1177 ERCPs, cholangitis occurred in 5% with 3 deaths (2).
In this case, there were just a couple of these dead areas, and I don’t think that the decedent would have died when he did were it not for the fact that he was a train wreck waiting to happen going in, He had >95% stenosis of his LAD, end stage COPD, etc. In my opinion this sepsis was a final stressor on his cardiovascular system, and triggered a sudden cardiac death (for a good discussion, see Willich’s article)(3)).
You may ask “Hey Bill, why isn’t there a cool picture of the gallbladder?” The answer is because I made a boo-boo. When I looked at the gallbladder, it was distended (had about 150cc of bile) and a few stones, but didn’t look all that thickened like the chronic cholecystitis cases i’m used to. So I didn’t think to get a section. I was thinking this was just a cardiac death and sailed right past it. When I found the necrotic bit of the liver, I didn’t think to go back and grab a piece. Total brain fart. I ended kicking myself in the head when I sat down to write up the case. I had to infer that there was a pneumococcal cholecystitis from the fact that it had to go through point A to get to point B, but I should have done better. No excuses. I don’t think it hampered the interpretation or determination of cause and manner of death, but it left a few strings loose at the end. Sigh.
As always, free for use in lectures, etc. with or without attribution, though attribution is appreciated. Higher resolution images available upon request.
- Thosani, N., Zubarik, R.S., Kochar, R., Kothari, S., Sardana, N., Nguyen, T. and Banerjee, S., 2016. Prospective evaluation of bacteremia rates and infectious complications among patients undergoing single-operator choledochoscopy during ERCP. Endoscopy, 48(05), pp.424-431.
- Christensen, M., Matzen, P., Schulze, S. and Rosenberg, J., 2004. Complications of ERCP: a prospective study. Gastrointestinal endoscopy, 60(5), pp.721-731.
- Willich, S.N., Maclure, M., Mittleman, M., Arntz, H.R. and Muller, J.E., 1993. Sudden cardiac death. Support for a role of triggering in causation. Circulation, 87(5), pp.1442-1450.
Great case, thanks!
Steve Cohle