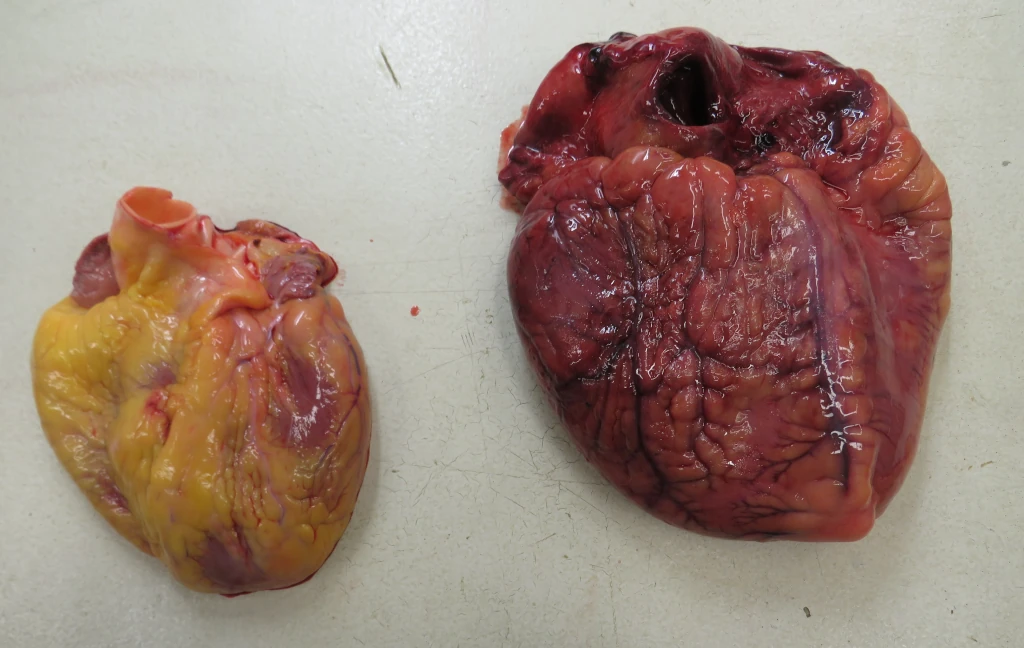
This is the case of a 33 year old woman who collapsed while walking to the kitchen. At autopsy, she weighed 662 lbs. Her heart weighed 993 grams, and displayed severe 4 chamber dilation. There was pulmonary edema and centrilobular congestion of the liver. Her medical history was remarkable for “obesity hypoventilation syndrome” which I learned as “Pickwickian syndrome” of hypoventilation, chronic hypoxia, and hypercapnia. When I was a medical student, we were taught that this was primarily due to the work of breathing associated with so much chest fat, but nowadays it seems to be multifactorial.
Here’s a gross photo of the decedent’s heart next to a “more” normal heart of a person who died that day of trauma. Note two things. First, the “more” normal heart is also enlarged — coming in at about 450 grams. It turns out I had three autopsies that day, and all were large people with large hearts. The second thing to notice is that the larger heart looks a bit on the decomposed side. This is often a problem with super morbidly obese folk. The large amount of body fat acts as insulation; even if you get the body refrigerated quickly, the internal organs cool so lowly they can show significant decompositional change if the body is in the fridge overnight.
Back when I was a student, there was not a specific thing called “obesity cardiomyopathy,” but it seems to be popular now as a diagnosis. As one review notes(1):
The nomenclature “obesity cardiomyopathy” refers to cardiac morphological, functional, and metabolic abnormalities originating from obesity alone . In some cases, the term “metabolic cardiomyopathy” may be used in reference to the broad setting of metabolic disorders including insulin resistance, diabetes mellitus, and obesity. In general, long-term obesity is closely associated with cardiac remodeling, characterized as LV hypertrophy, cardiac fibrosis, and diastolic dysfunction that eventually evolves to overt heart failure. [Internal references redacted].
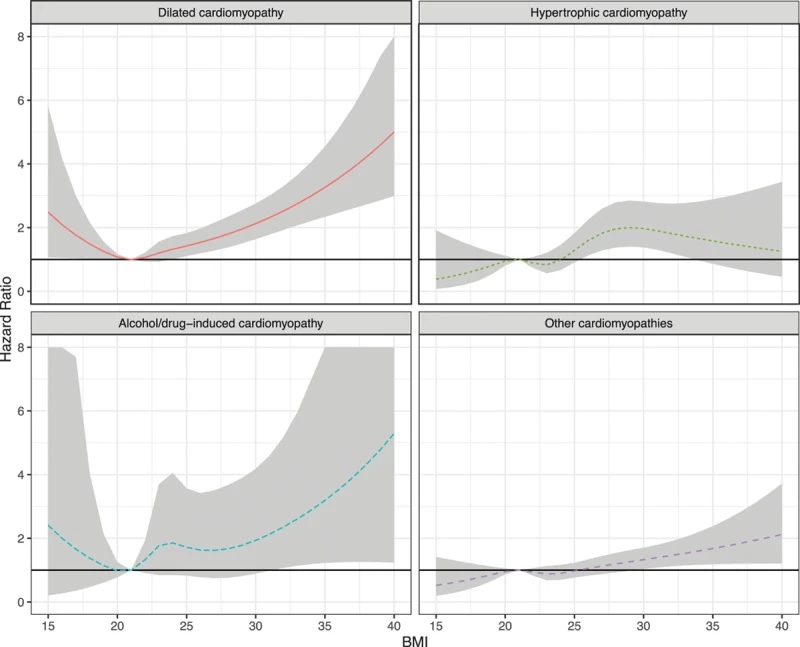
Here’s a graph of the hazard ratios of cardiomyopathy correlated with BMI from a study of Swedish women:
I should also point out that there’s this thing called the “obesity paradox” where people who are obese with heart failure tend to have a lower mortality than matched people without obesity. That’s different than getting heart failure in the first place. Some folk have said that the “obesity paradox” is a statistical anomaly due to selection and other biases. I don’t know.
- Ren, J., Wu, N.N., Wang, S., Sowers, J.R. and Zhang, Y., 2021. Obesity cardiomyopathy: evidence, mechanisms, and therapeutic implications. Physiological reviews, 101(4), pp.1745-1807.
- Robertson J, Lindgren M, Schaufelberger M, Adiels M, Björck L, Lundberg CE, Sattar N, Rosengren A, Åberg M. Body mass index in young women and risk of cardiomyopathy: a long-term follow-up study in Sweden. Circulation 141: 520–529, 2020. doi:10.1161/CIRCULATIONAHA.119.044056.